Dr Dhananjay performed first zero contrast angioplasty of Bihar and Jharkhand when it was started to grooming in India, the concept was well analysed and accepted in its early years. He was using routine IVUS imaging since long but the challenge was to analyse the slow flow and no flow phenomenon without contrast. For this he had to study imaging in detail, travel to multiple places to observe and got advanced imaging training from prof Gary Minz ( USA ) & Dr Akiko Maehara ( USA) in early 2023. This gave him the perfect idea to analyse the flow dynamics even in the absence of contrast.
Zero-contrast angioplasty, also called ultra-low contrast PCI when only a minimal amount of contrast is used, is an advanced interventional technique in which coronary angioplasty and stenting are performed without injecting iodinated contrast dye. Its primary purpose is to prevent or significantly reduce the risk of contrast-induced acute kidney injury (CI-AKI), particularly in patients with advanced Chronic Kidney Disease, a single functioning kidney, prior contrast nephropathy, severe heart failure with associated renal dysfunction, or those nearing dialysis dependency. Contrary to common misconception, this is not a “blind procedure.” It is a highly sophisticated, image-guided intervention that depends on meticulous planning, operator expertise, and detailed knowledge of coronary anatomy.
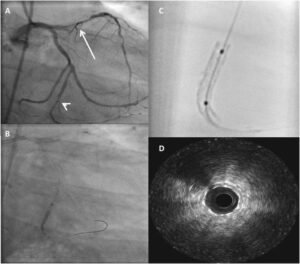
The procedure begins with careful review of a previously performed coronary angiogram, which serves as a detailed roadmap for understanding vessel course, lesion characteristics, branch points, and ideal stent landing zones. During the intervention, guidewires are advanced into the target vessel and often into side branches, creating fluoroscopic landmarks that help orient the operator throughout the procedure. The cornerstone of zero-contrast PCI is extensive use of Intravascular Ultrasound, which provides real-time visualization of the vessel lumen and wall, enabling precise assessment of vessel diameter, lesion length, plaque morphology, calcium burden, and optimal stent sizing. Although Optical Coherence Tomography may occasionally be used, its reliance on contrast injection limits its utility in true zero-contrast interventions.
Stent deployment is then guided using fluoroscopic wire markers, calcific landmarks visible under fluoroscopy, and the previously mapped anatomy. Final optimization is performed using IVUS to confirm adequate stent expansion, proper apposition, and complete lesion coverage, ensuring procedural success without the need for contrast injection. This technique represents a major advancement in contemporary interventional cardiology, allowing safe and effective coronary revascularization in high-risk renal patients while preserving residual kidney function.